
|
As an optometrist with a strong interest in preventing short-sightedness progression in children, it's not uncommon for me to have to explain to frustrated and sometimes even angry parents who have come to see me for a second opinion after receiving incorrect, misleading or conflicting advice from other optometrists about ways to manage their children's eyes from getting worse. Their frustration is completely understandable. Most parents want the best for their children, and that includes their eyesight. And most parents will trust the advice and information provided by their optometrist during their children's eye tests. Unfortunately, sometimes that trust is misplaced. I have had parents tell me that other optometrists never advised them there was any way to prevent their kids' eyes from worsening each year with increasing short-sightedness (myopia). For some parents, despite voicing their concerns that their children's eyes were deteriorating at a rapid rate every 6-12 months, were simply told to accept this as being a 'normal' part of growing up and that was nothing that could be done except to update their lenses to a stronger prescription. As a result of being misguided by their optometrists, many of these children have developed moderate to high myopia at a young age. One girl I saw recently, in particular, is now over -10.00D short-sighted at just age 16, with exponentially higher risks of developing a retinal detachment, glaucoma and other eye diseases for the rest of her life. Eye growth and the eye health risks associated with progressive myopia cannot be reversed. Even laser surgery will not help as the eye's internal layers are physically stretched and thinned. If only someone had told them about myopia control before. For these patients to feel let down by their previous optometrists is entirely justified. It's time to think about short-sightedness as more than simply a condition involving glasses. Myopia is, in fact, an eye health condition. One with potentially serious complications if let to progress on its own. Glasses and contact lenses merely mask the underlying condition by making vision clearer. 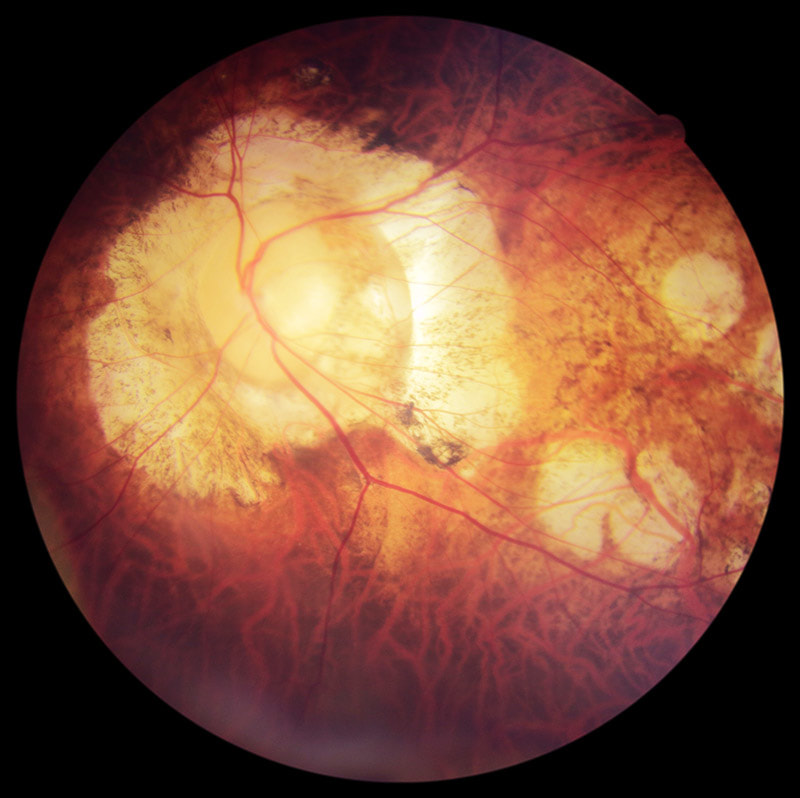 A patient with high myopia seen at this clinic recently. This patient has unfortunately developed vision loss from glaucoma & myopic macular degeneration associated with his high degree of short-sightedness. Myopia control had not been available when he was growing up. This is 2018, not 1990. Short-sightedness is a preventable condition today and has been for several years. Progressive vision deterioration in children and teenagers with myopia can be slowed down with clinically effective, evidence-based treatments. Optometrists who do not discuss myopia management strategies with the parents of children developing myopia are, in my view, failing to provide proper clinical care. And any optometrist who suggests "there's nothing that can be done to slow myopia progression in children" is either lying, incompetent, or at worst, negligent. The published clinical research papers on myopia control are widely available, and as eye care professionals all optometrists owe their patents a duty of care to provide the best care based on the best knowledge available. Ignorance is not a defence. My approach in this clinic is to give every child a full assessment of their visual functions and an analysis of their myopia progression and risk profile. I explain what this means to their parents and give them my professional recommendations based on the latest research applicable to their child's situation. I allow ample consultation time for parents to understand the information presented and to answer any questions they may have. For more challenging cases, I also reach out to world-renowned myopia experts on an international forum to discuss the appropriate management approach. My aim is always to ensure that parents are empowered with the knowledge to make a properly informed decision for their child's eyes.  Thick prescription lenses to correct high myopia — this can now be prevented with appropriate myopia control treatment. Here are some of the reasons why I think many optometrists in Australia today still do not discuss myopia control with their patients, or provide conflicting information:
LACK OF KNOWLEDGE Despite the availability of published evidence to support myopia management options for children, including effectiveness statistics of the various treatment strategies, many optometrists are unaware of these studies, or are lacking in their understanding of how to apply the relevant research data to clinical practice. Granted, myopia management is not a simple area of practice and is constantly evolving as new research is published. Keeping fully up-to-date demands attention and time. Many of the theories and knowledge surrounding myopia development and progression are also complex, that optometrists who are not specially interested in the subject matter may find it too complex to understand and to apply. BUSINESS MODEL It is unfortunate that many of today's optometrists operate under corporate business models that prioritise the selling of glasses over providing thorough clinical eye care. Pushed to see an many customers as possible, optometrists in these retail settings generally have shorter allocated consultation times of just 15-20 minutes (compared to 40 minutes at this clinic), which is often inadequate to perform highly detailed children's vision assessments, let alone discuss the available treatment options with the parents. Many optometrists working in retail-focused glasses stores consider myopia management as 'too difficult' and 'too time-consuming', therefore preferring to take the easy way out which is to simply prescribe a new pair of stronger glasses for their patients and send them on their way. Also, these corporate practices tend to employ many different optometrists, each with varying levels of skills, experience and knowledge, which inhibits proper continuity of care between visits when a patient may see a different optometrist each time and potentially may receive different, conflicting advice from one practitioner to the next. BIASED RECOMMENDATIONS An optometrist can only recommend to their patients services and products that they can offer in their practice. This is one reason why some parents receive contradictory advice at different practices while seeking a second opinion. For example, not all optometrists are therapeutically endorsed, which means they may not be qualified to prescribe medical treatments such as atropine eye drops for myopia control. Other optometrists may not have the technology or the expertise to fit Ortho-K lenses. Many optometrists do not have access to MiSight 1 Day contact lenses as they are only available to selected practices. For these reasons an optometrist's recommendations may be biased by what he or she can offer, hence the sometimes inconsistent advice from one practice to another. Multifocal glasses — despite being the least effective form of myopia management strategy — are often recommended by optometrists who are unable to, or reluctant to, to offer their patients potentially more effective options (such as atropine, Ortho-K or dual-focus soft lenses). I would suggest that if a practitioner has a child with rapidly progressive myopia in their room but is unable to offer the best solutions to help control the child's progression, it is in the child's best interests to be referred to another practitioner who can. At a dedicated myopia management clinic such as this, where every evidence-based treatment strategy is available, patients can be sure that recommendations are unbiased. COMMERCIAL CONSIDERATIONS The selling of glasses forms a large part of an optometry practice's revenue. So consider for a moment the business implications of treating a child to prevent their eyes from getting worse — if their eyes don't get worse the optometrist doesn't get the opportunity to sell them a new pair of glasses or new lenses every 6-12 months! There is actually a financial disincentive for practices that build their business primarily on selling glasses to offer myopia control to their patients. Prescribing treatments instead of glasses would increase 'chair time', increasing the number of reviews that do not generate glasses sales. As eye care professionals, optometrists should offer what is in their patients' best interests, but unfortunately many practitioners are driven by meeting company KPI targets and attracted to lucrative bonuses to drive sales. As utterly selfish and unethical as that seems, regrettably that is the commercial reality in today's increasingly retail-driven health care environment that most optometrists find themselves in. A further point to consider is that when a patient's prescriptions increases with their progressive myopia, the cost of their glasses lenses also increase. Many retail optometrists capitalise on selling lens upgrades — high-index thin lenses — for their medium and high prescription patients. There are even KPI targets specifically on up-selling lens upgrades — I would know, having previously worked for corporate optometry stores at various stages of my career. Keeping a patient's prescription low with myopia management means reduced dispensing of expensive high-index lenses over the individual's lifetime. Multiply that by tens of thousands of patients, and millions around the world. You can start to see why many mainstream optometrists do not proactively recommend myopia control to prevent children's prescriptions from increasing — despite the obvious risks to their patients' eye health as their myopia progresses. They have commercial reasons not to. At Eyecare Concepts, you can be assured that commercial considerations never come before patient care. That is what sets us apart. Colour vision deficiency (CVD), or otherwise called colour blindness, is a fairly common condition in the population. Around 8% of males (1 in 12) have some level of deficiency in colour matching, and around 0.5% of females (1 in 200). It is mostly a hereditary eye condition through a gene carried on the X chromosome (passing from mother's side), resulting in an imbalance of the numbers and densities of colour receptor cells (cones) in an individual's retina. Our eyes have three types of cone photoreceptors cells (green, red and blue) to detect colour information in our vision. There are two main types of hereditary colour vision deficiency: deutan (green cone receptor deficient) or proton (red cone deficient). A third type, tritan (blue cone deficient), is usually an acquired rather than congenital condition and is very rare. In each of these types, an individual may have a mild deficiency (almost normal), a moderate or a severe colour vision defect (significant difficulty in differentiating between certain shades of colours). At Eyecare Concepts, in addition to the standard Ishihara colour vision screening test (coloured dots forming numbers on a page) that most optometrists use, we have a more detailed colour vision test known as the Farnsworth D-15 colour matching test. While the common Ishihara screening tool can detect the presence of a colour vision defect, it does not differentiate between the type of colour defect or its severity. With the Farnsworth D-15 test — which involves matching a series of coloured discs from one to the next in similarity — we can assess the type of colour vision deficiency (deutan, protan or tritan) and also grade the severity of the deficiency between normal-mild, medium or severe. This is important when colour vision assessment is required for certain vocations or career choices. If you or your child has a colour vision deficiency, or there is a known family history, see us for a more comprehensive colour vision assessment test.  Farnsworth D-15 Test (left); Ishihara Test (right)  Farnsworth D-15 Test: Normal Colour Vision  Deutan (green receptor) Colour Vision Deficiency  Protan (red receptor) Colour Vision Deficiency  Tritan (blue receptor) Colour Vision Deficiency EYECARE CONCEPTS
FAMILY & CHILDREN'S OPTOMETRIST — MELBOURNE If you or your child is wearing Ortho-K sleep contacts and they aren't working as well as expected, perhaps we can help. Fitting Ortho-K lenses is much more complex than regular contact lenses and requires a high level of professional skill, expertise and technology to get right. At this practice I have seen some patients with Ortho-K lenses fitted by other practitioners who may not have the best equipment or knowledge, resulting in sub-optimal vision and unhappy experiences. Below is an example of a 9 year old girl (-4.00 short-sighted) who was fitted with Ortho-K lenses by another Melbourne practice. She had never been satisfied with her vision from her lenses, experiences a large drop in vision from morning to evening, and despite her previous optometrist trying 4 different sets of lenses from 3 lens manufacturers she was unable to achieve 20/20 vision, hindering her vision at school. So her mum decided to seek a second opinion. 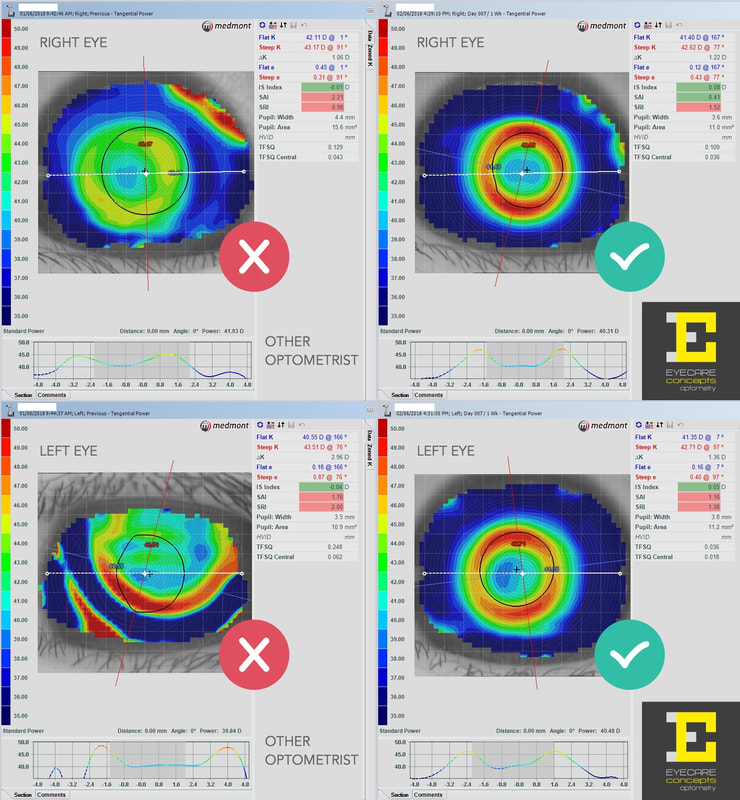 The right side images show the effect of well-centred lenses and defined treatment zones for good Ortho-K outcome. Left images show poorly fitted and de-centred Ortho-K lenses. At her first visit to this practice I measured her eye surface topography and it was quite obvious that her Ortho-K lenses were not fitting her eyes properly, hence the poor visual outcome and short treatment holding time during the day. Her treated vision was 20/40, that's 3 lines worse than 20/20 vision on the letter chart. Her lenses were unstable and de-centred on her eyes (especially the left eye) as she slept with her lenses on at night. Lens centration and treatment zone centration are key to achieving good results with Ortho-K. A well-centred Ortho-K lens places even pressure and forces across the eye surface for optimum moulding effect — essential for good vision and myopia control. I asked her to discontinue her lens wear for one week, by which time her cornea (the front surface of the eye) had completely reversed to its normal, non-treated shape. I then designed a new set of Ortho-K lenses for her using our advanced corneal topography technology and lens design software. This more sophisticated lens design approach allows me to create fully-customised lenses to suit all individual eye shapes and prescriptions. Having full control of every parameter of the lens shape, curvature and size means better fitting lenses and vision outcomes than older, trial lens-based Ortho-K fitting systems that some optometrists use. Within 2 weeks the new Ortho-K lenses were presented to her. At her first review, after one night of wear, she was already seeing better than her previous troublesome lenses, and one week later (when the above right-side topography maps were taken) she was achieving 20/20 vision and much happier with her vision at school. It is expected that the quality of her vision will improve further still as she wears her Ortho-K lenses into her second and third weeks and the corneal moulding and treatment zone areas stabilise. So a very happy patient and mum and well worth the visit to see us! Dr Philip Cheng — Melbourne Optometrist & Orthokeratologist
Member of the Orthokeratology Society of Oceania (OSO) |
AuthorPhilip Cheng - B.Optom (Melb) Ocular Therapeutics (GCOT). Optometrist at Eyecare Concepts Kew East, Melbourne. An experienced eye care & contact lens practitioner with expertise in myopia control & orthokeratology. Archives
August 2018
Categories
All
|
 RSS Feed
RSS Feed