
|
Myopia control is a hot topic in current eye research, in a bid to find the best ways of preventing and slowing vision deterioration for today's generation of children growing up in our tech-filled world. Many studies have been conducted globally in the past several years to analyse and compare the effectiveness of different treatment strategies available to reduce the progression of myopia ('short-sightedness') in children and adolescents. Naturally, different studies will report different findings and figures for treatment effectiveness, depending on variables such as sample size, subjects and study methodology. Here's how the current myopia control strategies stack up across multiple studies, in terms of the percentage reduction in the rate of myopia progression (eg. 0% = no effect in slowing progression; 100% = stops progression completely): Ortho-K corneal reshaping lenses: 32-100% Atropine eye drops (including low & high dose): 30%-77% Low-dose atropine eye drops: 59% Dual-focus & multifocal soft contact lenses: 29-70% Multifocal glasses for children with specific near focusing issues: 37% Multifocal glasses across all myopic children: 12-17% Regular single-vision glasses & contact lenses: 0-5% Due to the variability of the findings from different studies, and also individual variability from child to child from natural biological differences, this is generally what I recommend to parents seeking a myopia control opinion for their children: The best forms of myopia control treatment are currently Ortho-K overnight lenses, low-dose atropine eye drops, and dual-focus daytime soft contact lenses. Ortho-K and dual-focus contact lenses are optical treatments, and atropine eye drops is a pharmacological treatment; they work in different ways. As a guide, all three have an average effectiveness of around 50% in slowing the rate of childhood myopia progression. Some children achieve better myopia control than a 50% reduction, some may even stop progressing altogether, and others may need combination treatment to achieve the best control for their myopia. And some kids respond better to one type of treatment than another. What does a 50% reduction actually mean for my child? 50% reduction in myopia progression means we halve their prescription increase each year compared to no treatment or simply wearing standard single-vision glasses or contact lenses. For a child whose prescription is increasing rapidly at -1.00 per year, that reduces to -0.50 per year with myopia control treatment. While it may not sound like much, it is hugely significant over a longer timeframe. Over an eight-year period, for example, from age 8 to 16, if a child's myopia increases at a average rate of -1.00 per year (the actual rate may be faster some years and less other years), this child could have -8.00 degree of myopia at age 16. Halving the progression means he or she has -4.00 of myopia instead. There is a significant difference in the child's lifelong eye heath risks between having -4.00 and -8.00 of myopia. The risks of eye diseases associated with high myopia, such as retinal detachment and myopic macular degeneration, increase exponentially rather than linearly. Halving the degree of myopia from -8.00 to -4.00 reduces the risk of retinopathy (diseases of the retina) by a factor of 10, as the following graph illustrates. 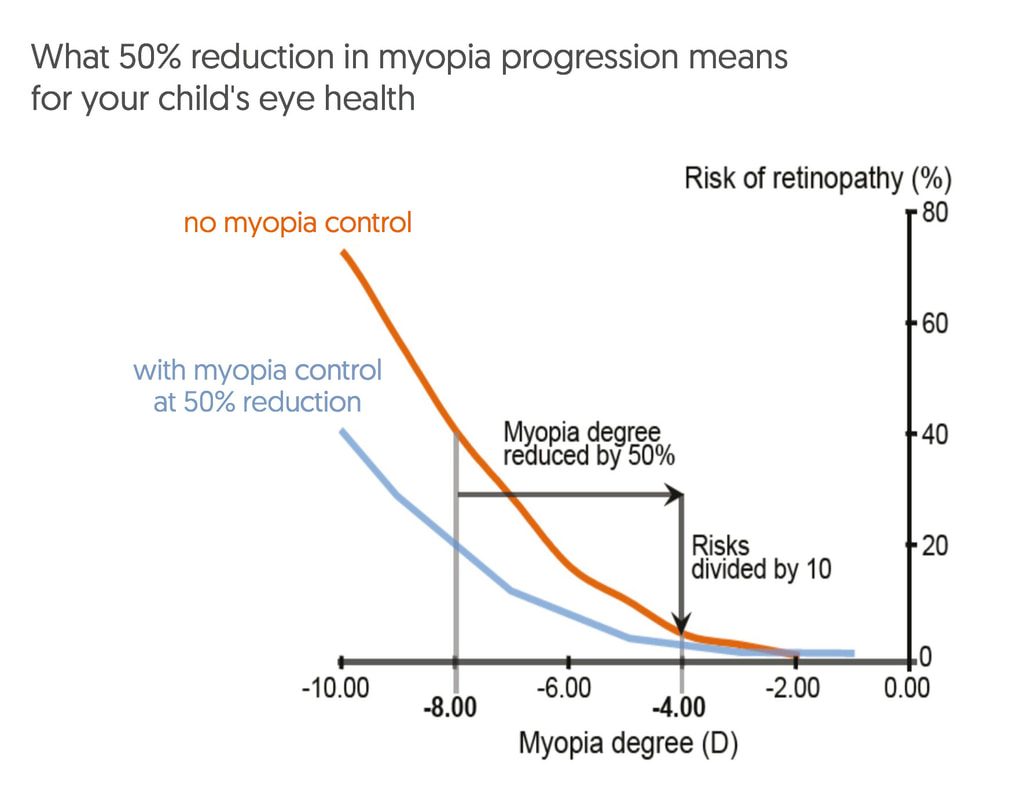 For more information about myopia control treatment options, visit our dedicated website at www.themyopiaclinic.com.au
EYECARE CONCEPTS · THE MYOPIA CLINIC MYOPIA CONTROL OPTOMETRIST — MELBOURNE As an optometrist with a strong interest in preventing short-sightedness progression in children, it's not uncommon for me to have to explain to frustrated and sometimes even angry parents who have come to see me for a second opinion after receiving incorrect, misleading or conflicting advice from other optometrists about ways to manage their children's eyes from getting worse. Their frustration is completely understandable. Most parents want the best for their children, and that includes their eyesight. And most parents will trust the advice and information provided by their optometrist during their children's eye tests. Unfortunately, sometimes that trust is misplaced. I have had parents tell me that other optometrists never advised them there was any way to prevent their kids' eyes from worsening each year with increasing short-sightedness (myopia). For some parents, despite voicing their concerns that their children's eyes were deteriorating at a rapid rate every 6-12 months, were simply told to accept this as being a 'normal' part of growing up and that was nothing that could be done except to update their lenses to a stronger prescription. As a result of being misguided by their optometrists, many of these children have developed moderate to high myopia at a young age. One girl I saw recently, in particular, is now over -10.00D short-sighted at just age 16, with exponentially higher risks of developing a retinal detachment, glaucoma and other eye diseases for the rest of her life. Eye growth and the eye health risks associated with progressive myopia cannot be reversed. Even laser surgery will not help as the eye's internal layers are physically stretched and thinned. If only someone had told them about myopia control before. For these patients to feel let down by their previous optometrists is entirely justified. It's time to think about short-sightedness as more than simply a condition involving glasses. Myopia is, in fact, an eye health condition. One with potentially serious complications if let to progress on its own. Glasses and contact lenses merely mask the underlying condition by making vision clearer. 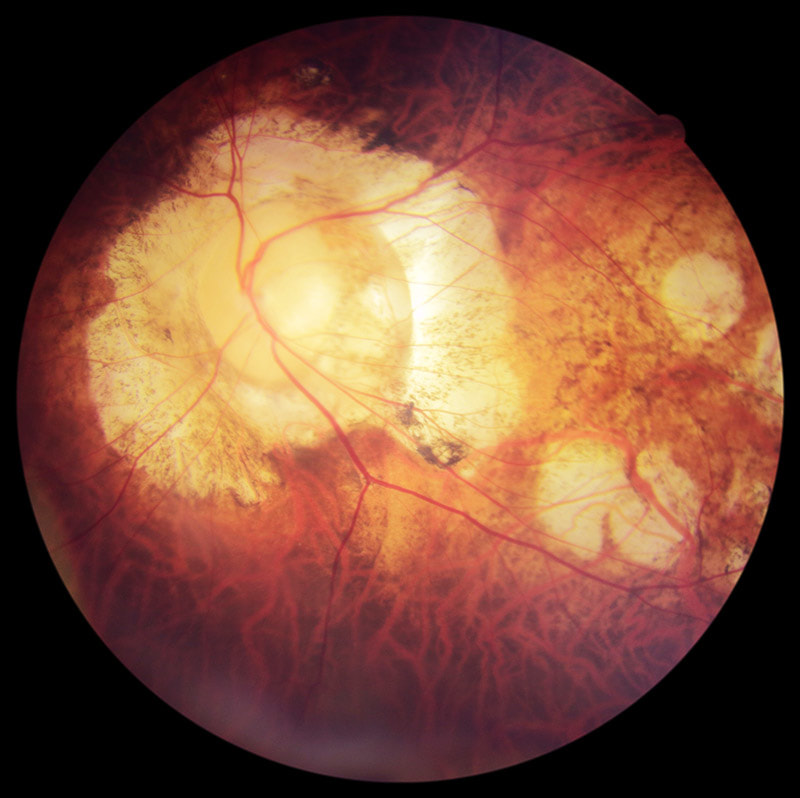 A patient with high myopia seen at this clinic recently. This patient has unfortunately developed vision loss from glaucoma & myopic macular degeneration associated with his high degree of short-sightedness. Myopia control had not been available when he was growing up. This is 2018, not 1990. Short-sightedness is a preventable condition today and has been for several years. Progressive vision deterioration in children and teenagers with myopia can be slowed down with clinically effective, evidence-based treatments. Optometrists who do not discuss myopia management strategies with the parents of children developing myopia are, in my view, failing to provide proper clinical care. And any optometrist who suggests "there's nothing that can be done to slow myopia progression in children" is either lying, incompetent, or at worst, negligent. The published clinical research papers on myopia control are widely available, and as eye care professionals all optometrists owe their patents a duty of care to provide the best care based on the best knowledge available. Ignorance is not a defence. My approach in this clinic is to give every child a full assessment of their visual functions and an analysis of their myopia progression and risk profile. I explain what this means to their parents and give them my professional recommendations based on the latest research applicable to their child's situation. I allow ample consultation time for parents to understand the information presented and to answer any questions they may have. For more challenging cases, I also reach out to world-renowned myopia experts on an international forum to discuss the appropriate management approach. My aim is always to ensure that parents are empowered with the knowledge to make a properly informed decision for their child's eyes.  Thick prescription lenses to correct high myopia — this can now be prevented with appropriate myopia control treatment. Here are some of the reasons why I think many optometrists in Australia today still do not discuss myopia control with their patients, or provide conflicting information:
LACK OF KNOWLEDGE Despite the availability of published evidence to support myopia management options for children, including effectiveness statistics of the various treatment strategies, many optometrists are unaware of these studies, or are lacking in their understanding of how to apply the relevant research data to clinical practice. Granted, myopia management is not a simple area of practice and is constantly evolving as new research is published. Keeping fully up-to-date demands attention and time. Many of the theories and knowledge surrounding myopia development and progression are also complex, that optometrists who are not specially interested in the subject matter may find it too complex to understand and to apply. BUSINESS MODEL It is unfortunate that many of today's optometrists operate under corporate business models that prioritise the selling of glasses over providing thorough clinical eye care. Pushed to see an many customers as possible, optometrists in these retail settings generally have shorter allocated consultation times of just 15-20 minutes (compared to 40 minutes at this clinic), which is often inadequate to perform highly detailed children's vision assessments, let alone discuss the available treatment options with the parents. Many optometrists working in retail-focused glasses stores consider myopia management as 'too difficult' and 'too time-consuming', therefore preferring to take the easy way out which is to simply prescribe a new pair of stronger glasses for their patients and send them on their way. Also, these corporate practices tend to employ many different optometrists, each with varying levels of skills, experience and knowledge, which inhibits proper continuity of care between visits when a patient may see a different optometrist each time and potentially may receive different, conflicting advice from one practitioner to the next. BIASED RECOMMENDATIONS An optometrist can only recommend to their patients services and products that they can offer in their practice. This is one reason why some parents receive contradictory advice at different practices while seeking a second opinion. For example, not all optometrists are therapeutically endorsed, which means they may not be qualified to prescribe medical treatments such as atropine eye drops for myopia control. Other optometrists may not have the technology or the expertise to fit Ortho-K lenses. Many optometrists do not have access to MiSight 1 Day contact lenses as they are only available to selected practices. For these reasons an optometrist's recommendations may be biased by what he or she can offer, hence the sometimes inconsistent advice from one practice to another. Multifocal glasses — despite being the least effective form of myopia management strategy — are often recommended by optometrists who are unable to, or reluctant to, to offer their patients potentially more effective options (such as atropine, Ortho-K or dual-focus soft lenses). I would suggest that if a practitioner has a child with rapidly progressive myopia in their room but is unable to offer the best solutions to help control the child's progression, it is in the child's best interests to be referred to another practitioner who can. At a dedicated myopia management clinic such as this, where every evidence-based treatment strategy is available, patients can be sure that recommendations are unbiased. COMMERCIAL CONSIDERATIONS The selling of glasses forms a large part of an optometry practice's revenue. So consider for a moment the business implications of treating a child to prevent their eyes from getting worse — if their eyes don't get worse the optometrist doesn't get the opportunity to sell them a new pair of glasses or new lenses every 6-12 months! There is actually a financial disincentive for practices that build their business primarily on selling glasses to offer myopia control to their patients. Prescribing treatments instead of glasses would increase 'chair time', increasing the number of reviews that do not generate glasses sales. As eye care professionals, optometrists should offer what is in their patients' best interests, but unfortunately many practitioners are driven by meeting company KPI targets and attracted to lucrative bonuses to drive sales. As utterly selfish and unethical as that seems, regrettably that is the commercial reality in today's increasingly retail-driven health care environment that most optometrists find themselves in. A further point to consider is that when a patient's prescriptions increases with their progressive myopia, the cost of their glasses lenses also increase. Many retail optometrists capitalise on selling lens upgrades — high-index thin lenses — for their medium and high prescription patients. There are even KPI targets specifically on up-selling lens upgrades — I would know, having previously worked for corporate optometry stores at various stages of my career. Keeping a patient's prescription low with myopia management means reduced dispensing of expensive high-index lenses over the individual's lifetime. Multiply that by tens of thousands of patients, and millions around the world. You can start to see why many mainstream optometrists do not proactively recommend myopia control to prevent children's prescriptions from increasing — despite the obvious risks to their patients' eye health as their myopia progresses. They have commercial reasons not to. At Eyecare Concepts, you can be assured that commercial considerations never come before patient care. That is what sets us apart. If you have eyesight problems with short-sightedness (myopia) there's a good chance your children will develop the same vision issues as they grow up. Statistically there's a 3 times risk of a child having myopia if one parent is myopic, and 6 times risk if both parents are myopic. Genetics is certainly a strong predisposing factor for myopia development. We can't do much about the genetic makeup of your child, but we can reduce the risk of your child having short-sighted eyes, or worse, highly short-sighted eyes — a condition known as 'high myopia', conventionally defined as myopia with a glasses prescription of -6.00 or over (600 degrees +). Many people, particularly of Asian descent, have even higher levels of myopia. -10.00 and above (1000 degrees short-sighted) are not uncommon. The highest we have seen in our practice is -16.00. Not only is having high myopia hugely inconvenient (nothing in front of your nose is clear without glasses) but the risks of developing serious eye diseases and blindness are exponentially higher. Previously there wasn't a lot that could be done to slow down short-sightedness progression. But now there is, and all parents should know about these options available to preserve your child's eyesight. With the current medical and optical treatments no child today should grow up to have high myopia anymore. Early intervention and treatment is key to maintaining good eyesight. Treatments and strategies to prevent children's eyes from getting worse with myopia is called 'myopia control'. Our myopia control clinic website (www.kidsorthok.com.au) goes into more detail about all the current options available to manage childhood myopia. Here is a summary: REGULAR EYE TESTS We recommend all children have yearly eye tests from the age of 3. Kids' eyes can change quickly and often without symptoms. Early detection of vision problems means earlier intervention. Undiagnosed and uncorrected short-sightedness can accelerate progression. And if there is significant progression, myopia control treatment should be initiated as early as possible. We monitor children with myopia progression every 6 months. ORTHOKERATOLOGY (ORTHO-K) Ortho-K are overnight lenses that correct vision while your child sleeps. The two benefits of OK lenses are: (1) They correct your child's eyesight so that daytime glasses and regular contact lenses are not needed for them to see. This gives them complete freedom for all their schooling, sports and recreational activities without worrying about breaking or losing glasses or contacts. (2) They are clinically effective in slowing down your child's eyesight deterioration by around 50%, and sometimes more. OK lenses work by gently reshaping the front surface of the eye with individually designed oxygen-permeable lenses that fit precisely on your child's eyes. You can think of orthokeratology as a little like orthodontic braces for align teeth. Over time the surface of the eye, the cornea, is molded to the shape of the lens to correct vision as well as provide myopia control. Some parents have concerns about safety of overnight contacts. Wearing contact lenses of all kinds carry potential risks of infection, but any significant adverse events with diligent Ortho-K wear are actually very rare. Studies have demonstrated that Ortho-K lenses for kids are no more risky than overnight wear of soft lenses by adults. OK lenses are worn at home under parental supervision, without the risk of contamination outside. Professionally fitted lenses, good hygiene and proper lens care will help ensure your child maintains healthy eyes wearing Ortho-K lenses. At our clinic we have any no episodes of infection or adverse events for our patients treated with OK lenses. MYOPIA CONTROL SOFT CONTACTS LENSES There are now daily-disposable soft contact lenses that help slow myopia progression. As these lenses are replaced daily after each use, without any need for cleaning or storage, they are the safest type of contact lenses and ideal for kids and teenagers. We have the MiSight 1 Day with ActivControl Technology available at our clinic. This lens was developed specifically for short-sighted children to prevent eye deterioration. These soft contact lenses are a 'multifocal' design with a clear distance zone in the middle, and a different power in the periphery of the lens. This mimics the effect of Ortho-K in modifying the focusing of light in the peripheral zone of the eye's surface. One key difference is that MiSight lenses are only effective while the lens is worn, so it needs to be worn at least 6 days a week, whereas the eye surface changes that occur with Ortho-K are longer-lasting and holds its myopia control effect even with occasional short breaks from overnight lens wear. OK lenses can also correct mild to moderate levels of astigmatism, while MiSight lenses are not available with astigmatism correction. ATROPINE EYE DROPS Atropine is a chemical agent that helps prevent myopia progression by strengthening the structures within the eyeball to resist eye growth and elongation that occurs concurrently with adolescent growth spurts. Although atropine has long been known to exhibit this effect, it wasn't routinely prescribed for myopia control due to its known potential side-effects on the eye and elsewhere in the body — eg. pupil dilation, light sensitivity, headache, stinging, dry mouth, dry skin, heightened irritability and increased heart rate. In the past 5 years, researchers discovered that even tiny concentrations of atropine, thus much safer to use, can effectively help modulate myopia progression almost as well as the full-dose form. This low-dose 0.01% atropine is just 1/100th of the original atropine concentration. 0.01% atropine eye drops are very well tolerated in kids with minimal side-effects as a long-term treatment. In our clinic we have prescribed this treatment for children as young as 4 and have had good results. We have also combined atropine treatment with Ortho-K or soft contact lenses for even greater myopia control effect in some children with more aggressive progression. MYOPIA CONTROL SPECTACLE LENSES Regular single vision glasses do not help to prevent myopia progression. There are special children's glasses specifically developed for myopia control. Although clinical research shows that glasses in general are not as effective forms of myopia control compared to the other options described above, they are nonetheless still beneficial for some children, and better than wearing ordinary glasses or no treatment at all. The myopia control spectacle lenses available from our clinic are the Essilor Myopilux lenses — developed originally for short-sighted children in Singapore and Hong Kong. These were special bifocal or progressive lenses and most effective for children with some near focusing difficulties or inefficiencies. Our optometrist will assess your child's eye focusing system to determine if he or she could benefit from wearing this type of lens. REGULAR BREAKS FROM NEAR WORK Near work — which includes reading, drawing, study, homework, tutoring and computer use — is an essential part of your child's schooling and education. Many children are required to use an iPad or laptop computer at school. This is no avoiding digital technology that are intrinsic to our modern lives. We recommend following the 20/20/20 rule in regards to near work. That means for every 20 minutes of concentrated near focusing, take 20 seconds to look at something in the far distance 20 metres away. That helps your child to relax their eyes periodically. Also, children should always keep their books at least an elbow's distance away from their eyes when reading. SPENDING MORE TIME OUTDOORS If you child has been tested and found to have normal eyesight, the best you can do to preserve their good vision and potentially delay the onset of myopia is to let them spend more time outdoors in bright light. This is good scientific evidence that more outdoor time helps to prevent against myopia development. Ambient outdoor light is many magnitudes brighter than indoor light, and is believed to help modulate proper eye growth. We recommend all children spend at least 90 minutes a day participating in outdoor activities. If you have concerns about your child's eyes or would like to know more about our myopia control program, book a comprehensive kids' vision assessment with our experienced myopia control optometrist today.  Philip Cheng — Myopia Control Children's Optometrist · 墨爾本兒童視光師 EYECARE CONCEPTS · THE MYOPIA CLINIC Kew · Balwyn · Balwyn North Today, more children in Australia and around the world are developing short-sightedness (myopia) and from an earlier age. But thankfully we can now slow childhood short-sightedness progression and help prevent high myopia with effective treatments which weren't available a generation ago. As one of Melbourne's leading myopia control optometrists, many of the kids who come to our practice have parents who have high myopia themselves (some as high as -10.00 to -16.00) and understandably very concerned about their children's eyesight growing up. Myopia is, at least in part, a hereditary condition. Children with both parents having myopia have a 6 times risk of developing short-sightedness, and more severely. So at what age can we start myopia treatment for your child? There is no age requirement for starting myopia control treatment. We recommend starting treatment as soon as we have identified that your child is at high risk of developing high myopia (> -6.00) in the future. This reduces your child's lifelong risks of glaucoma, retinal detachment and myopic macular degeneration — diseases with a potential for blindness. Here at Eyecare Concepts, we have prescribed myopia control treatment for children as young as 3 years of age. Which children are in the high-risk category for myopia? Younger children, those at age 7 or under at the time of being first diagnosed with short-sightedness, are at highest risk. And the younger the child, the greater the risk — there is more time for the eyeball to grow and elongate as the child grows through the years of adolescence and puberty. We also analyse individual data for each child to determine their rate of myopia progression per year. A documented myopia increase of -1.00 or more in a 12 month period is considered rapid progression that should be treated. Is it possible to predict if a child will become short-sighted? Yes, it is possible to make predictions based on a child's current level of refractive error. Generally, across the population, a normal 3 year old child should be long-sighted by around +2,00, a 4 year old around +1.50 and a 6 year old around +1.00. Long-sightedness acts as a buffer to prevent short-sightedness in a normally-developing eye. If we identify that your child is less long-sighted than is normal for his or her age, your child has a greater risk of developing short-sightedness and needs to be monitored more closely. For example, a child who is only +0.25 long-sighted at age 4 has a very high myopia risk, especially if this child has other risk factors such as genetics. There are specific tests we do to accurately measure the refractive status of a young child. Can we prevent the onset of myopia with treatment? Recent studies have shown that spending more time outdoors (for at least 90 minutes a day) has a protective effect on the eye and can prevent or delay the onset of childhood short-sightedness. For children who are not yet short-sighted but are at risk, we prescribe an increase in outdoor time as a preventative measure. Low-dose atropine treatment is highly effective in slowing progression once a child is already short-sighted, but there is little clinical data at present on its effect for myopia prevention in children with normal eyesight. There is some suggestion that it can indeed prevent myopia onset. We would assess the possibility of prescribing low-dose atropine for myopia prevention in a child without myopia on a case-by-case basis by weighing up the potential benefits vs risks. Certain glasses may help children who have difficulties with near focusing and eyestrain that can increase their risk of myopia development. Binocular vision testing is part of the comprehensive children's vision assessment in our clinic to identify these at-risk children. If you have questions about myopia control treatments for your child, please contact our clinic. EYECARE CONCEPTS · THE MYOPIA CLINIC
MELBOURNE MYOPIA CONTROL OPTOMETRIST — KEW · KEW EAST · BALWYN A common question that we have had from parents is where can they buy 0.01% atropine eye drops? Low-dose atropine is a highly effective treatment strategy to slow short-sightedness progression in children and teenagers, with very low risks of side effects, and is one that we at Eyecare Concepts prescribe regularly as part of our SightControl program for myopia control. While regular-dose atropine eye drops (1% concentration) are readily available as a prescription medicine in pharmacies, this concentration is not commonly used for myopia control as the potential side effects and adverse reactions in the eye and also in the body are considered too high to be used long-term. 0.01% atropine eye drops are essentially a diluted formulation (1/100th concentration) of the regular 1% atropine, and at this very low concentration it is a much safer treatment for young children. This low-dose form is not currently commercially available in Australia — although there are whispers that some pharmaceutical companies are working to make this available in due course, such is the growing need for effective myopia control for children worldwide. At the present time 0.01% atropine is only available as a compounded medicine — that means it is formulated by a compounding chemist and bottled individually on order. The compounding chemist must also be one certified and suitably equipped to produce sterile bottles of eye drops, without risk of possible contamination that could lead to infection. Optometrists are, by Australian law, unable to dispense prescription-only eye drops directly to patients.  Commercially made 0.01% atropine eye drops like this are available in some countries, but not currently in Australia. GETTING A PRESCRIPTION FOR LOW-DOSE ATROPINEIn Australia, 0.01% atropine does NOT necessarily need to be prescribed by an eye specialist (an ophthalmologist). A therapeutically-endorsed optometrist with an interest in myopia control can prescribe this low-dose atropine treatment for your child. Please also note that if you have a prescription from overseas for a child already using low-dose atropine treatment for myopia control, you will need a new prescription issued in Australia to purchase the eye drops here, as overseas prescriptions cannot be accepted. As an experienced, therapeutically-endorsed optometrist with expertise in myopia control, our optometrist can assess your child's myopia, prescribe low-dose atropine treatment and manage his/her myopia progression without the need see an eye specialist first. We can even measure your child's eye length to monitor eye growth and progression. This is a bulk billing clinic and a referral is not required. COMPOUNDING CHEMISTSConveniently located near our Kew East practice, Pharmacy Smart Compounding in Balwyn (with another branch in East Melbourne) is a compounding chemist that we recommend to our local patients. Each bottle of eye drops, priced at around $36, has an expiry of 1 month after opening and an unopened shelf life of 3 months. A discount may be available for a dual pack (2 months of treatment). Occasionally they may have pre-made bottles in stock, otherwise a new bottle takes around 2 days to prepare. For patients outside of Melbourne we can give recommendations of interstate compounding pharmacies able to supply 0.01% atropine eye drops for postal delivery. Please contact our practice for further details. USING LOW-DOSE ATROPINE EYE DROPSLow-dose atropine eye drops are administered one drop per day, in each eye, at night before sleep. Your child's regular glasses and/or contact lenses are to be worn as usual to see. An initial one-month trial of the eye drops is recommended for children first starting treatment, to ensure the medication is well tolerated by your child and that there are no unexpected sensitivity or adverse events. While the medication is safe it is still a chemical agent going in your child's eyes. Some children report a very slight increase in glare sensitivity. After a successful first month, it may be more economical to purchase a bulk supply (2 to 6 months) at a time instead of single bottles. TREATMENT REVIEWS Children on low-dose atropine for myopia control need to be monitored on a regular basis. When we issue a prescription for atropine treatment we take on the responsibility of managing your child's myopia and eye health. We review children with myopia progression every 6 months and tailor their treatment according to their rate of progression. An increase of atropine dosage to 0.02% or 0.05% (also need to be compounded), or a change to another form of myopia control therapy, such as Ortho-K and MiSight lenses, or combination treatment, are sometimes required for kids who do not respond well to 0.01% atropine alone. Every child is different, and some children's myopia progression are more challenging to manage. Besides low-dose atropine, all other current evidence-based treatments for myopia control in children are available at Eyecare Concepts. You may also visit our myopia clinic's dedicated Myopia Clinic website for further information. If you have any questions about 0.01% atropine eye drops please call us on (03) 9819 7695, or click below to book a consultation for your child. EYECARE CONCEPTS
MELBOURNE MYOPIA CONTROL OPTOMETRIST — KEW · KEW EAST · BALWYN Updated 25/6/2018 We are delighted to the one of the first optometrists in Australia to be accredited to prescribe the new CooperVision MiSight 1 Day soft lens designed specifically to slow short-sightedness progression in children and teenagers.
Effective myopia control is now available in a safe, hygienic, daily disposable soft contact lens suitable for short-sighted children of all ages. This lens can reduce sight deterioration and myopia progression in children by around 50% - that means a -1.00 per year prescription increase can be halved to -0.50, significantly reducing the risk of developing high myopia (> -6.00) over time as the child grows up. We believe this lens is a game-changer in myopia management and we are excited to have this product made available to our patients, as another option in our SightControl program prescribed at our practice. |
AuthorPhilip Cheng - B.Optom (Melb) Ocular Therapeutics (GCOT). Optometrist at Eyecare Concepts Kew East, Melbourne. An experienced eye care & contact lens practitioner with expertise in myopia control & orthokeratology. Archives
August 2018
Categories
All
|
 RSS Feed
RSS Feed