
|
Myopia control is a hot topic in current eye research, in a bid to find the best ways of preventing and slowing vision deterioration for today's generation of children growing up in our tech-filled world. Many studies have been conducted globally in the past several years to analyse and compare the effectiveness of different treatment strategies available to reduce the progression of myopia ('short-sightedness') in children and adolescents. Naturally, different studies will report different findings and figures for treatment effectiveness, depending on variables such as sample size, subjects and study methodology. Here's how the current myopia control strategies stack up across multiple studies, in terms of the percentage reduction in the rate of myopia progression (eg. 0% = no effect in slowing progression; 100% = stops progression completely): Ortho-K corneal reshaping lenses: 32-100% Atropine eye drops (including low & high dose): 30%-77% Low-dose atropine eye drops: 59% Dual-focus & multifocal soft contact lenses: 29-70% Multifocal glasses for children with specific near focusing issues: 37% Multifocal glasses across all myopic children: 12-17% Regular single-vision glasses & contact lenses: 0-5% Due to the variability of the findings from different studies, and also individual variability from child to child from natural biological differences, this is generally what I recommend to parents seeking a myopia control opinion for their children: The best forms of myopia control treatment are currently Ortho-K overnight lenses, low-dose atropine eye drops, and dual-focus daytime soft contact lenses. Ortho-K and dual-focus contact lenses are optical treatments, and atropine eye drops is a pharmacological treatment; they work in different ways. As a guide, all three have an average effectiveness of around 50% in slowing the rate of childhood myopia progression. Some children achieve better myopia control than a 50% reduction, some may even stop progressing altogether, and others may need combination treatment to achieve the best control for their myopia. And some kids respond better to one type of treatment than another. What does a 50% reduction actually mean for my child? 50% reduction in myopia progression means we halve their prescription increase each year compared to no treatment or simply wearing standard single-vision glasses or contact lenses. For a child whose prescription is increasing rapidly at -1.00 per year, that reduces to -0.50 per year with myopia control treatment. While it may not sound like much, it is hugely significant over a longer timeframe. Over an eight-year period, for example, from age 8 to 16, if a child's myopia increases at a average rate of -1.00 per year (the actual rate may be faster some years and less other years), this child could have -8.00 degree of myopia at age 16. Halving the progression means he or she has -4.00 of myopia instead. There is a significant difference in the child's lifelong eye heath risks between having -4.00 and -8.00 of myopia. The risks of eye diseases associated with high myopia, such as retinal detachment and myopic macular degeneration, increase exponentially rather than linearly. Halving the degree of myopia from -8.00 to -4.00 reduces the risk of retinopathy (diseases of the retina) by a factor of 10, as the following graph illustrates. 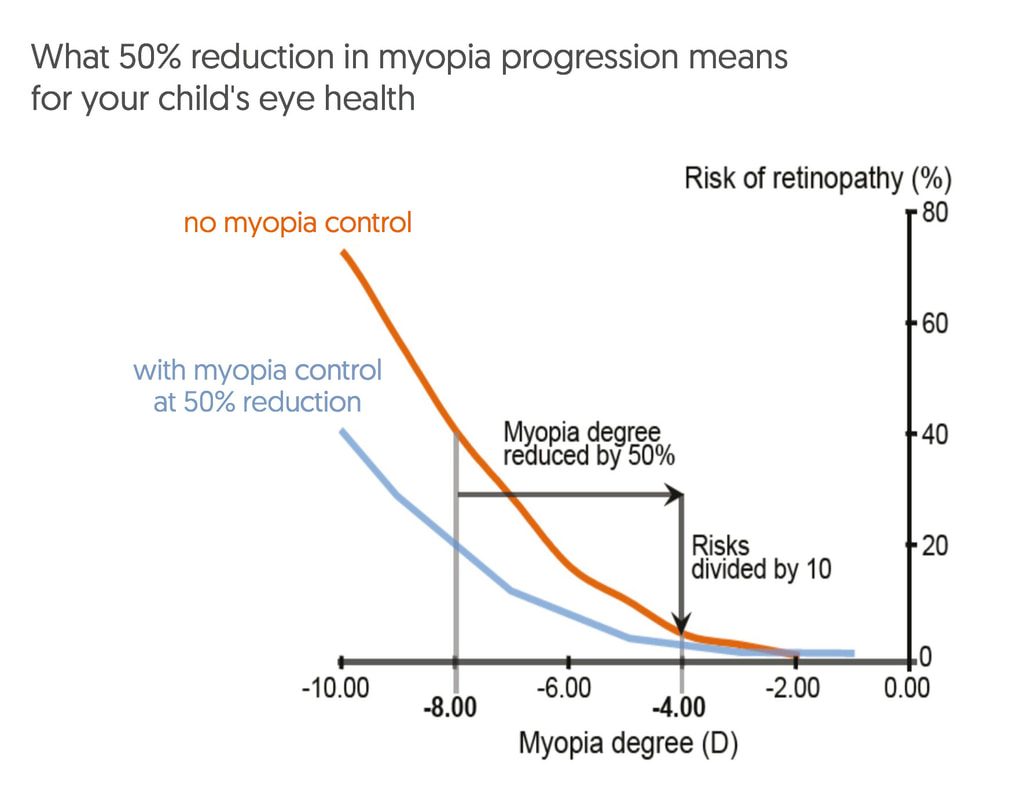 For more information about myopia control treatment options, visit our dedicated website at www.themyopiaclinic.com.au
EYECARE CONCEPTS · THE MYOPIA CLINIC MYOPIA CONTROL OPTOMETRIST — MELBOURNE |
AuthorPhilip Cheng - B.Optom (Melb) Ocular Therapeutics (GCOT). Optometrist at Eyecare Concepts Kew East, Melbourne. An experienced eye care & contact lens practitioner with expertise in myopia control & orthokeratology. Archives
August 2018
Categories
All
|
 RSS Feed
RSS Feed